
State Choices to Promote Access
[2016]3
- Children <1 year
Sets eligibility at 319% (S-CHIP) and 220% (Medicaid) - Children 1-5 years
Sets eligibility at 319% (S-CHIP) and 162% (Medicaid) - Children 6-18 years
Sets eligibility at 319% (S-CHIP) and 138% (Medicaid and M-CHIP) - Pregnant women
Sets eligibility at 220% (Medicaid)
- [2014]4
- [2014]4
- Provides temporary coverage to pregnant women under Medicaid until eligibility can be formally determined [2018]5
- Provides temporary coverage to children under Medicaid or CHIP until eligibility can be formally determined [2018]5
- Includes at-risk children in the definition of eligibility for IDEA Part C [2014]6
- Does not require redetermination of eligibility for Medicaid/CHIP more than once a year [2018]5
- Has adopted Medicaid expansion as part of the Affordable Care Act [2018]7
State Choices to Promote Quality
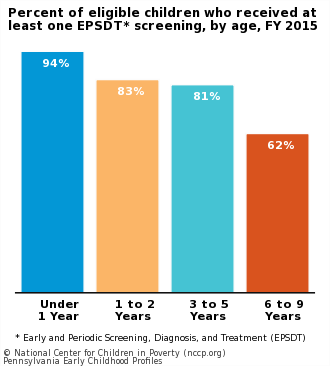
EPSDT screening periodicity schedule meets recommendations of American Academy of Pediatrics [FY 2016]2
- 7 screenings for children <1 year
State requires 6 screens. 100% of eligible screens were completed in 2016. - 4 screenings for children 1-2 years
State requires 5 screens. 100% of eligible screens were completed in 2016. - 3 screenings for children 3-5 years
State requires 3 screens. 100% of eligible screens were completed in 2016. - 4 screenings for children 6-9 years
State requires 4 screens. 80% of eligible screens were completed in 2016.
- Requires newborn screening for the 31 metabolic deficiencies/disorders and core conditions [2014]8
30 universally required by law or rule.
Data Notes and Sources
Last Updated: October 29, 2015
Send us recent developments to update your state's profile.
- National data were calculated from the 2011 American Community Survey, representing information from 2011. State data were calculated from the 2009-2011 American Community Survey, representing information from the years 2009 to 2011.
- U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services. (2017). The Annual EPSDT Report (Form CMS-416) for FY 2016. https://www.medicaid.gov (accessed December 11, 2017). Data were not reported for ND.
- Brooks, T., Miskell, S., Artiga, S., Cornachione, E., & Gates, A. (2016). Medicaid and CHIP Eligibility, Enrollment, Renewal, and Cost-Sharing Policies as of January 2016: Findings from a 50-State Survey. Kaiser Commission on Medicaid and the Uninsured, The Henry J. Kaiser Family Foundation. Http://files.kff.org (accessed February 29, 2016).
- Medicaid. 2014. Medicaid and CHIP Coverage of Lawfully Residing Children and Pregnant Women. http://medicaid.gov (accessed August 25, 2015).
- Brooks, T., Miskell, S., Artiga, S., Cornachione, E., & Gates, A. (2018). Medicaid and CHIP Eligibility, Enrollment, Renewal, and Cost-Sharing Policies as of January 2018: Findings from a 50-State Survey. Kaiser Commission on Medicaid and the Uninsured, The Henry J. Kaiser Family Foundation. http://files.kff.org (accessed July 2, 2018).
- Ringwalt, S. (Comp.). (2015). Summary table of states' and territories' definitions of/criteria for IDEA Part C eligibility. http://www.nectac.org (accessed August 25, 2015).
- Kaiser Commission on Medicaid and the Uninsured. (2018). Status of State Action on the Medicaid Expansion Decision. https://www.kff.org (accessed July 13, 2018).
- National Newborn Screening and Genetics Resource Center. 2014. National Newborn Screening Status Report. http://genes-r-us.uthscsa.edu (accessed March 24, 2015).